
You have exactly 900 seconds.
That is the average length of a standard endocrinology appointment. In those 15 minutes, you are expected to summarize 2,160 hours of life, 1,800+ medical decisions, and several thousand data points from your CGM.
Most of the time, it goes like this: You sit on the crinkly paper, the nurse takes your vitals, the doctor glances at your A1C, asks "How are you feeling?", you say "Fine," they renew your prescriptions, and you’re back in the parking lot feeling like nothing actually changed.
The "Fine" Trap is where real progress goes to die. If you want to stop guessing and start solving the variables that actually make your life hard, you have to treat your endo appointment like a high-level consulting session, not a parent-teacher conference.
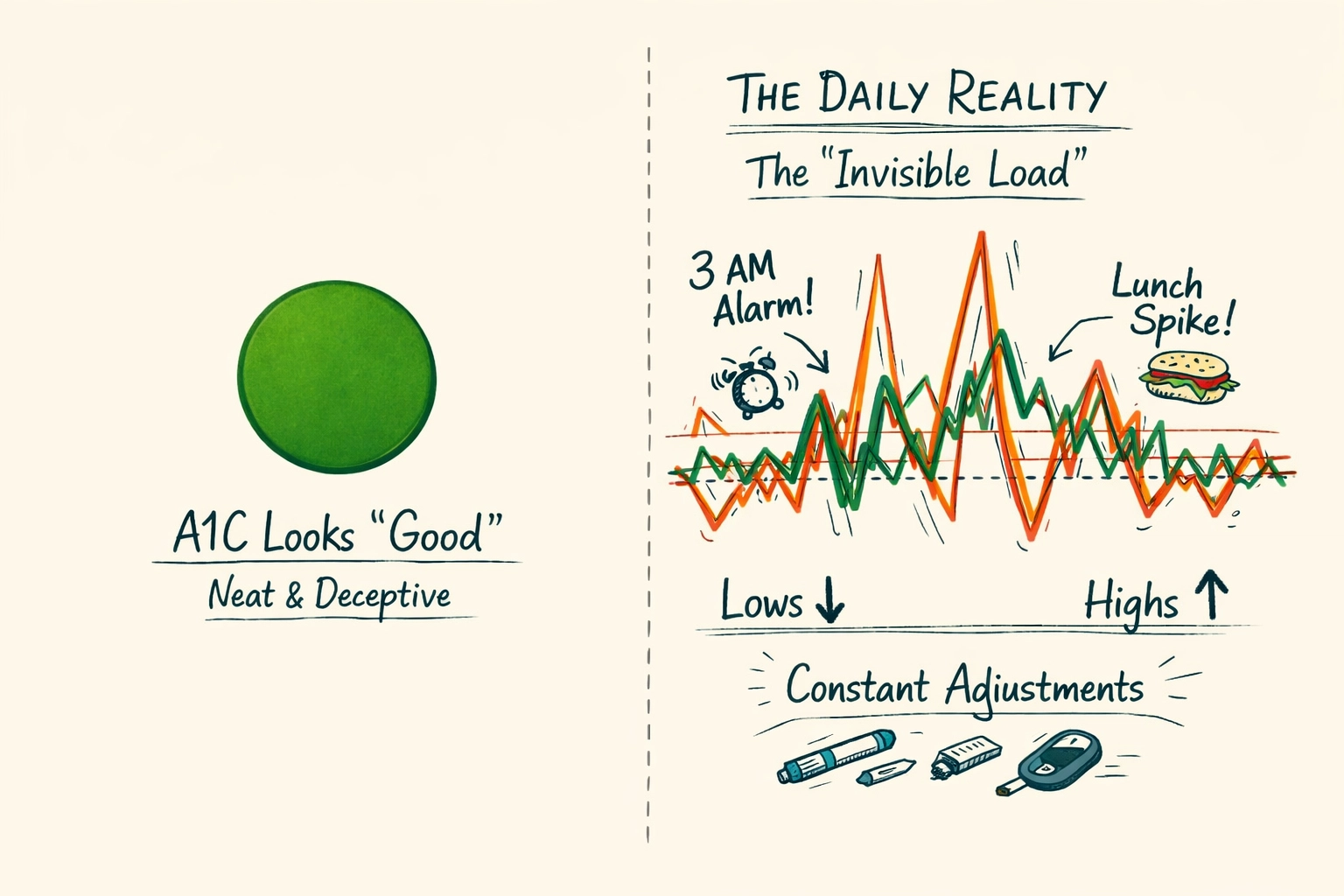
There is a specific kind of performance we all do in the clinic. We want to be the "good patient." We want the gold star. We focus on the A1C because it’s a single, tidy number that makes the doctor smile.
But the A1C is a liar. It’s a three-month average that hides the 3 AM rage-boluses, the post-work spikes, and the crushing exhaustion of "diabetes burnout."
When you tell your doctor you’re "fine" because your A1C is 6.8, you are leaving the invisible load on your own shoulders. You’re essentially telling your consultant that the business is profitable while ignoring the fact that the warehouse is on fire.
Your endo cannot fix what they cannot see. If you walk in and say, "I’ve been running high lately," you’ve given them a symptom, not a cause. To get an answer in 15 minutes, you need to provide a diagnostic.
Stop relying on the endo to scroll through your pump or CGM history during the session. They are looking for patterns, but they don't live your life. They don't know that Tuesday's spike was a high-stress board meeting and Thursday's low was a broken sensor.
Do an audit 48 hours before you arrive:
When you speak the language of data and context, you move the conversation from "try harder" to "let's adjust the basal rate."
That is a passive question. It puts the doctor in the role of a judge. Instead, ask high-leverage, technical questions that force a strategic adjustment.
If you are using tools like Subseven to track the "why" behind your numbers, you already have the insights. Your goal in the appointment is to get the clinical "green light" to tweak your system.
Try these instead:
These questions demonstrate that you understand the mechanism. They move you from "patient" to "collaborator."

T1D is 10% biology and 90% cognitive load. Yet, mental health is often the first thing cut from a 15-minute window.
Many of us feel that bringing up "burnout" or "fatigue" sounds like complaining. It isn’t. It’s clinical data. If you are too exhausted to log your carbs or check your CGM, your management will fail regardless of how perfect your ratios are.
How to bring it up:
"I am experiencing significant diabetes fatigue. It is affecting my ability to make the 180+ decisions required daily. I need to talk about strategies to reduce the cognitive load, whether that’s adjusting targets to be less aggressive for a month or trying a more automated system."
If your endo brushes this off with a "just keep at it," that is a signal. You might need a referral to a CDE (Certified Diabetes Care and Education Specialist) or a therapist who specializes in chronic illness.
Most people treat their endo as their primary point of contact for everything. But in the ecosystem of T1D, they have different roles:
If your 15-minute appointment feels too rushed for the "how-to" stuff, ask specifically: "Can you refer me to a CDE for a 60-minute session on exercise management?"

To ensure you don’t leave the office with that "I forgot to ask the main thing" feeling, use this checklist before you walk in.
At Subseven, we believe that the best management happens when you take the "stressing and guessing" out of the equation. That starts with realizing that you are the one living with the data 24/7.
Your endocrinologist is a highly skilled consultant. They have the clinical knowledge, but you have the lived experience. You are the CEO of your own biology.
When you walk into that room, don't wait for permission to speak or for them to find the patterns for you. Present your findings, ask for their clinical expertise on your proposed solution, and get back to your life.
The goal isn't to have a perfect appointment. The goal is to have a system that works so well you barely have to think about it between visits.

If you’re tired of the "guessing" part of the 15-minute appointment, it might be time to change how you track your data. Check out how we're making pattern recognition simple at subseven.ai/integrations.


